Emergency hospital admissions for COPD reached 121,129 in 2023/24, a 9% increase on the previous year. But the national average masks a stark postcode lottery: admission rates in South Yorkshire are five times higher than in parts of the Thames Valley. Our analysis explores where the burden falls hardest and what the data tells us about prevention.
Respiratory diseases affect one in five people and are the third leading cause of death in England, behind cancer and cardiovascular disease. The NHS Long Term Plan has identified respiratory disease as a clinical priority, and Chronic Obstructive Pulmonary Disease (COPD) is a major contributor to that burden.
COPD is a group of lung conditions, including emphysema and chronic bronchitis, that cause progressive breathing difficulties. It primarily affects middle-aged or older adults who smoke, and many individuals remain undiagnosed. The condition drives substantial hospital admissions, deepens health inequalities, and carries significant economic costs.
How many COPD emergency admissions are there in England?
Emergency hospital admissions for COPD are rising. In 2023/24, there were 121,129 emergency admissions, a 9% increase on the previous year. That translates to 208 admissions per 100,000 population. As The Guardian reported in November 2024, breathing issues now cause more emergency NHS admissions than any other condition.
Where are COPD admissions highest?
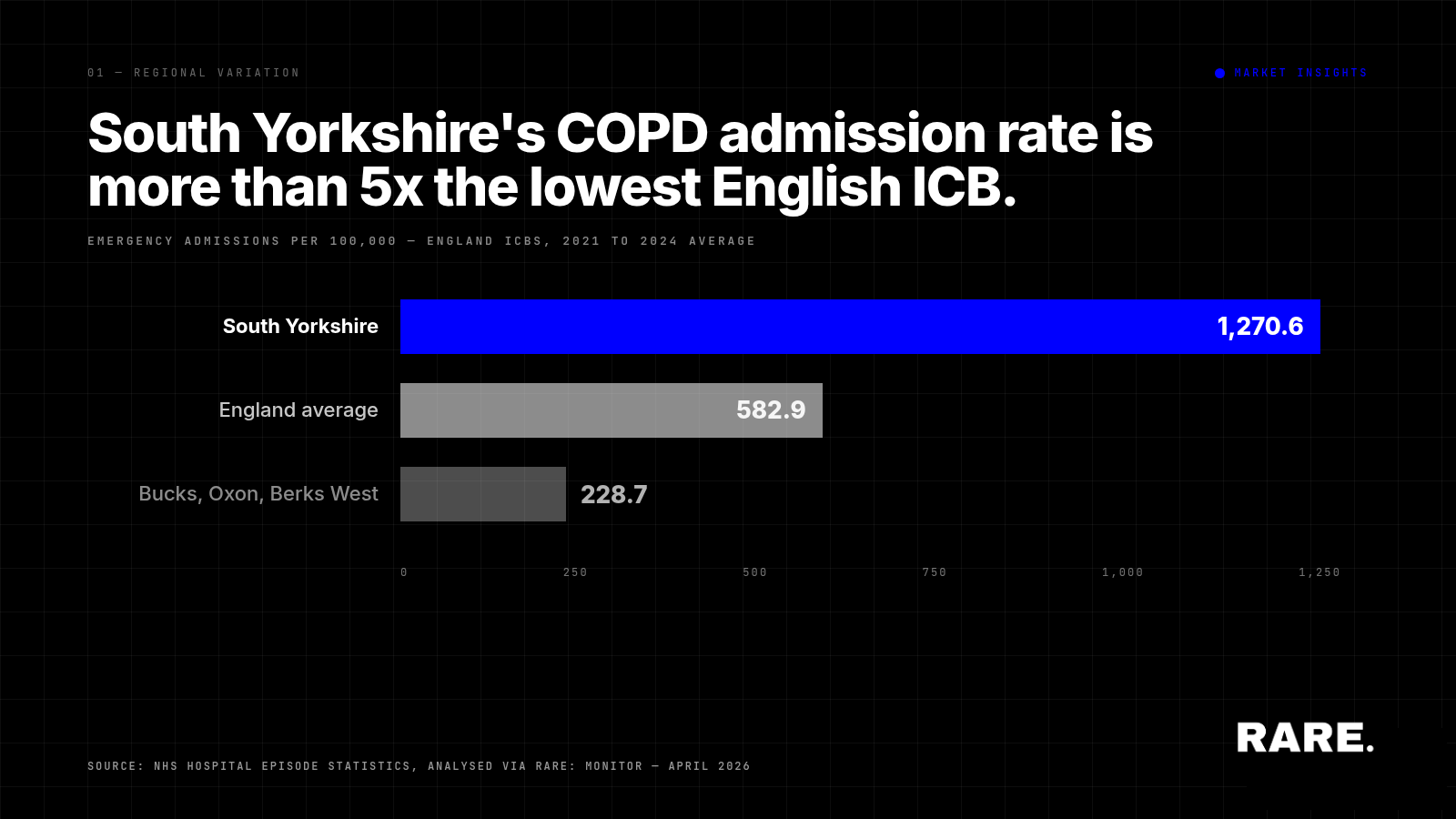
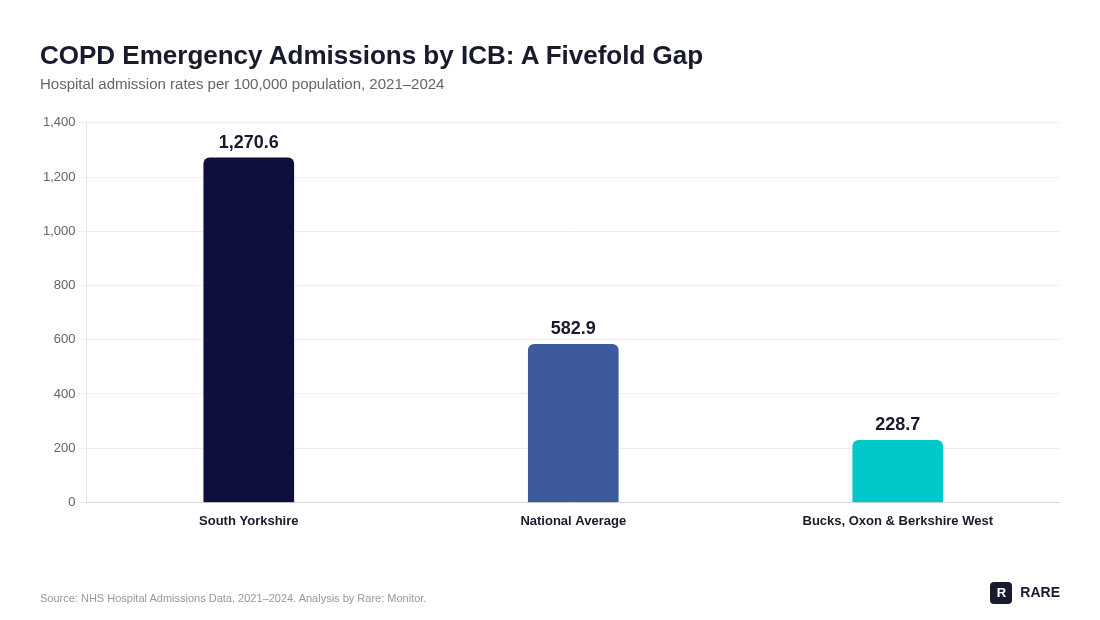
The national average masks enormous regional variation. Our analysis of hospital admissions data across England's Integrated Care Boards (ICBs) for the period 2021 to 2024 reveals a fivefold gap between the highest and lowest admission rates.
The national average was 582.9 admissions per 100,000 over the three-year period. But the South Yorkshire ICB recorded 1,270.6 per 100,000, more than double the national average. At the other end, the Buckinghamshire, Oxfordshire and Berkshire West ICB recorded just 228.7 per 100,000.
That gap raises questions about more than just disease prevalence. It points to differences in primary care capacity, smoking cessation support, air quality, deprivation, and early intervention.
How does deprivation drive COPD outcomes?
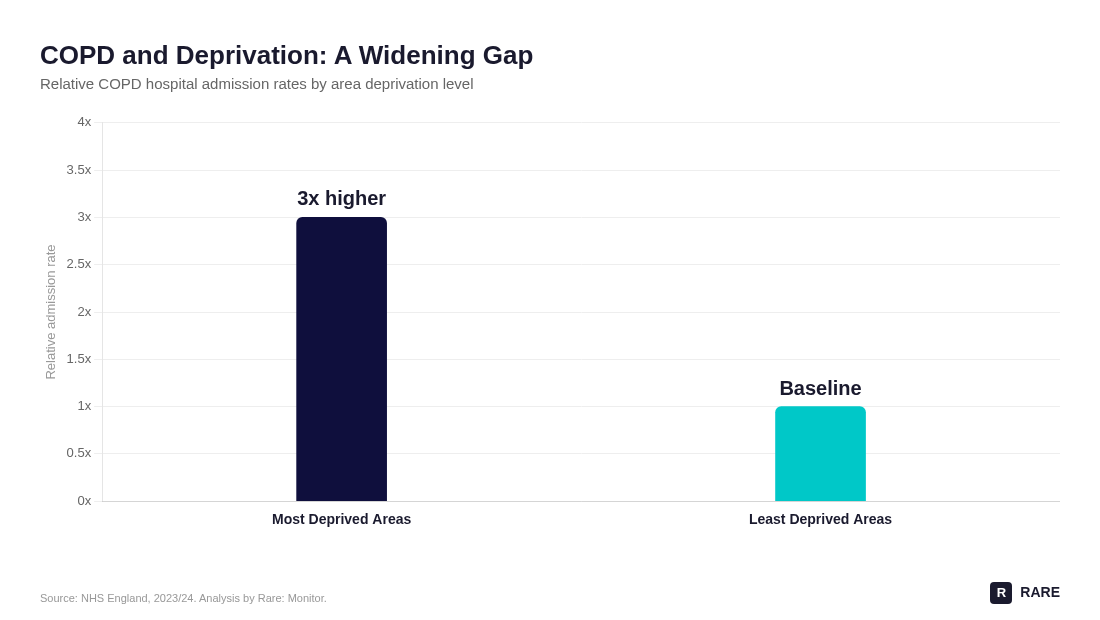
COPD disproportionately affects deprived communities, where smoking rates, air pollution exposure, and poor housing are higher. People in the most deprived areas experience hospital admission rates three times higher than those in the least deprived areas. This disparity is now wider than at any point on record.
The correlation between deprivation and COPD burden is not new. What is notable is that the gap continues to widen, suggesting that existing interventions are not reaching the communities that need them most.
What does prescribing data reveal about regional differences?
The variation extends into prescribing practices. Analysis of long-acting bronchodilator prescribing at ICB level shows significant differences in cost per capita across England.
The NHS Cheshire and Merseyside ICB had the highest indicative cost per capita for these treatments, while the NHS Gloucestershire ICB had the lowest. These differences reflect a combination of disease prevalence, prescribing culture, and formulary choices across regions.
What role can primary care play in reducing COPD admissions?
GP survey data from 2024 shows that the NHS South Yorkshire ICB has both the highest average percentage of the GP population reporting a lung problem (10.78%) and the highest rate of secondary care admissions (921.1 per 100,000) for the period 2021 to 2024.
Within South Yorkshire, some GP practices have particularly high proportions of patients reporting lung conditions. This raises a practical question: what can be done at GP level to reduce reliance on secondary care?
Smoking is the leading cause of COPD, and stopping at any stage is the most effective way to prevent its onset or slow its progression. Continued smoking accelerates lung function decline, while quitting reduces airway inflammation, preserves remaining lung capacity, and lowers the risk of flare-ups. Even long-term smokers see measurable benefits from cessation.
Support for quitting provided in general practice is especially effective. GPs can offer trusted advice, prescribe evidence-based treatments, and use regular patient contact to reinforce motivation. These interventions are shown to significantly increase quit rates.
Twenty-one COPD hotspots with no smoking cessation services
Across England, 21 locations have GP populations where more than 13% of registered patients have a lung condition, but no smoking cessation services are listed in the service directories that patients and clinicians use. These are the areas where COPD risk is most concentrated and where prevention provision is least visible.
The NHS Long Term Plan’s respiratory objectives depend on closing this kind of geographic gap, not on adding services where they already exist. The data points to where targeted intervention would land hardest.